

Search results
Search conducted in the four main databases yielded 28,018 records, and additional 21 records were produced from Google, Google scholar and institutional repositories. Thus, 28,039 records were produced from the search conducted. With the help of the Mendeley software, 1,311 duplicate records were removed and the remaining 26,728 records were screened. Abstracts and irrelevant records were removed from further screening leaving 134 full-text records for further assessment. A search through the reference lists of the selected full-text articles produced additional eight, and one record was obtained through consultation with the Digital Librarian (Dr. Kwame Kodua-Ntim). Thus, a total of 143 records were assessed for eligibility. Finally, 75 records were excluded using the eligibility criteria presented in Table 1, whereas 68 records were included in this review. Figure 1 presents the PRISMA flow diagram of the screening process. Most of the excluded studies did not report on psychosocial work factors which made it difficult to be considered in the study though they studied commercial drivers. The exclusion in this study was not based on study appraisal since authors did not appraise the included studies. Language barrier also led to the rejection of two records that could have added to the strength of the evidence reported in this review.
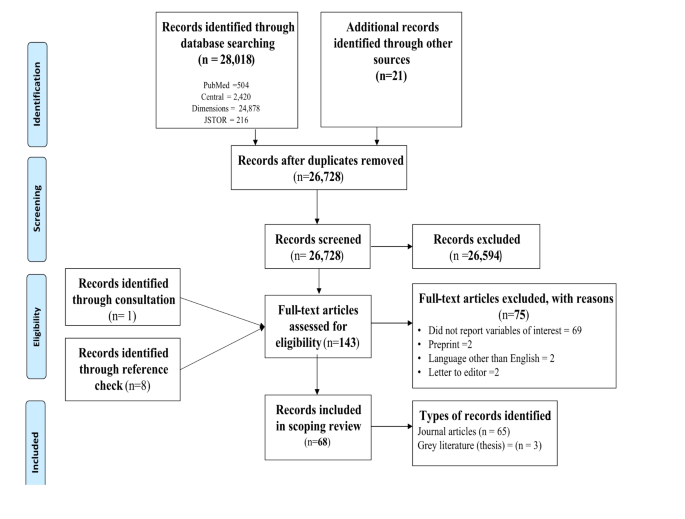
PRISMA flow diagram of screening process
Characteristics of reviewed studies
These 68 included studies were conducted in 32 countries across globally (See Fig. 2 for more details). United States leads with 9 studies, followed by Taiwan, 6 and Ethiopia, 4. Other countries, including Brazil, Canada, Mexico, the Netherlands, Spain, and Sweden, each contributed 3 studies. Countries like Australia, China, Colombia, Japan, South Africa, and the United Kingdom each conducted 2 studies, while a large number of countries, such as Argentina, Belgium, Chile, Denmark, Finland, Iran, Israel, Italy, New Zealand, Portugal, Saudi Arabia, Singapore, South Korea, Thailand, Turkey, Zambia, Zimbabwe have just 1 study each. The chart shows that cross-sectional surveys were the most frequently used research design, with 43 studies, followed by qualitative designs with 8 studies. Reviews and longitudinal designs each accounted for 5 studies, while both randomised controlled trials and mixed-method designs had 3 studies. Experimental design was the least common, used in just 1 study. This indicates a preference for observational and descriptive approaches in the reviewed studies (See details in Fig. 3). The studies sampled a total of 32,774 participants, including truck, taxi, bus and general commercial drivers (see supplementary file, Table S1).

Countries and continents where included studies were conducted

Methods/Designs of included studies
Psychosocial work factors of commercial drivers
The psychosocial work factors are grouped under three thematic areas (job design, organisational or workplace conditions and work environment).
Job design
Job design in the context of commercial drivers refers to the organisation of work tasks, demands, and available resources, balancing the physical and mental requirements of the job (such as long driving hours, time pressure, and workload) with supportive elements (like rest breaks, job control, and access to health resources) to ensure driver safety, well-being, and optimal performance [4]. Reviewed studies suggest that commercial drivers experience high job demands, making them vulnerable to fatigue and burnout [7, 11,12,13,14,15,16,17,18,19]. Thus, evidence shows that high physical workload [7, 20,21,22,23], long daily [9, 12, 22, 24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45], weekly [34, 37, 43, 46,47,48], driving hours, shift work [49, 50], time pressures [11, 24, 30,31,32, 51,52,53], social isolation [7, 8, 22, 39] and role overload [54] were inherent part of commercial drivers’ job that contribute to their poor health and well-being outcomes. Moreover, studies have reported that driving hours of more than 8 and 40 h a day and week, respectively, are harmful to commercial drivers’ health and road safety [9, 12, 25,26,27,28,29,30,31,32,33,34,35,36,37,38,39]. However, a study conducted on taxi drivers in Thailand reported that long daily driving more than 8 h a day was not associated with elevated haematocrit levels [55].
The argument is that organisations that prioritise health and well-being in designing jobs and make available job resources have the potential to alleviate the negative impacts of high job demands on commercial drivers. Thus, the lack of job resources to cope effectively with job demands may make commercial drivers vulnerable to occupational diseases [16]. For instance, studies have reported that low job control [7, 13,14,15, 17, 19, 51, 56, 57], work-family conflict [7, 30, 31, 51, 57, 58], poor remuneration [22, 24, 25, 27, 56], effort-reward imbalance [1, 12, 50, 59], lack of social support from co-workers [3, 7, 20, 39, 58] and supervisors [7, 51, 58, 60] and organisation support [51, 54] are markers for poor health, safety and well-being outcomes among commercial drivers. Studies that highlighted job strain, where the demands of the job outweigh the resources available to commercial drivers, also reported a negative impact on the drivers’ health and well-being [1,2,3, 8, 19, 59, 61, 62].
Organisation conditions
work conditions in the context of commercial drivers refer to the workplace environment and policies that shape their working experience, including job security, management support, safety regulations, working hours, scheduling of rest breaks, and access to essential resources like healthcare, sanitation, and social protection [2]. Evidence suggests that commercial drivers who perceive that their organisations prioritise profit or productivity over their well-being were more likely to report poor health outcomes [31, 51]. In addition, job insecurity in the road transport industry may predispose commercial drivers to occupational challenges [13, 22, 27, 56]. Furthermore, irregular work schedules [30, 31, 51, 52, 60], insufficient or lack of breaks and rest periods during driving hours [22, 26, 27, 34, 35, 42, 49, 57, 60, 63, 64], periodic breaks [65], lack of vacation [60, 65], lack of social protection such as insurance [22, 25] and poor organisational [24] and safety culture [9] may expose commercial drivers to occupational safety and health challenges. Moreover, lack of sanitation and exercise facilities at transport stations or yards may expose commercial drivers, especially those driving on standard routes, to chronic non-communicable diseases such as renal and cardiovascular conditions [7, 39, 52].
Work-environment
The work environment of commercial drivers refers to the physical, social, and operational conditions they encounter while driving, including road conditions, interactions with passengers and other drivers, and the availability of rest areas and supporting facilities [2]. The work environment of commercial drivers is often linked to experiences of hostile behaviours from passengers and other drivers [39, 60]. For instance, a qualitative study conducted among 55 commercial drivers in Chile mentioned confrontations from passengers as the leading cause of stress for drivers [60]. Also, studies have reported that conflict and violence like physical and verbal assault and robberies have exposed drivers to injuries, deaths and mental health challenges, including depression and post-traumatic stress disorder [3, 39, 43, 58].
Psychosocial working conditions and female commercial drivers
Three studies [39, 43, 58] reported on gender differences in exposure to psychosocial work factors among commercial drivers. One study found that working conditions are the same for male and female commercial drivers and, in many situations, that pose greater challenges for female drivers to cope in such a hostile work environment [43]. The other two studies exclusively sampled female commercial drivers from Mexico [39] and Southern Africa [58] and reported that long driving hours, lack of support from co-workers and supervisors, lone driving and work-family conflict expose female drivers to occupational health and safety challenges. Aside from the lack of social support, female commercial drivers experience various forms of abuse and harassment at the workplace, such as verbal assault, threats, homicide and sexual abuse [39, 58]. In addition, female commercial drivers have limited access to breaks and sanitation facilities [39]. These working conditions are precarious for women drivers in the road transport industry.
Psychosocial work factors of truck drivers
Results indicated that psychosocial work factors unique to truck drivers include irregular work schedules, often characterised by long hours, night shifts, and unpredictable working days, which disrupt their sleep patterns and overall health [7, 51, 52]. Additionally, unrealistic work schedules set by employers or clients may compel drivers to meet tight deadlines, increasing stress and fatigue [48]. Work-family conflict is another key factor, as truck drivers spend extended periods away from home, causing strain on personal relationships [30, 51]. Truck drivers often experience an increased need for recovery, as they may face physical and mental exhaustion from prolonged driving without sufficient rest [14, 64]. Additionally, the social isolation that truck drivers often encounter, spending extended hours alone on the road, may contribute to feelings of loneliness and a lack of social support, which can adversely impact their mental health and well-being [7, 8].
Impact of psychosocial work factors on health and well-being
Health implications of poor psychosocial work factors among commercial drivers were grouped into mental health, fatigue and sleep difficulties, musculoskeletal issues and injuries, non-communicable diseases and infectious, and other health issues.
Mental health issues
The link between precarious psychosocial working conditions and poor mental health or psychological distress is well documented [1,2,3, 8, 9, 24, 27, 31,32,33, 39, 50, 52, 56, 58]. Specifically, conditions such as depression [7, 8, 15, 22, 37, 47, 56, 57, 66], anxiety [7, 8, 15, 47], stress [7, 30, 60, 61], and PTSD [37] have been identified among commercial drivers who are exposed to job strain and hostile working environments. Lone driving, role overload, work-family conflict and lack of social support may lead to emotional exhaustion among commercial drivers [19, 54].
Fatigue and sleep difficulties
The link between long driving hours, job strain and sleep fatigue and daytime sleepiness has been reported [7,8,9, 29,30,31,32, 35, 37, 48, 49, 56, 58, 60, 67, 68]. In addition, commercial drivers who face high job demands without adequate recovery time are more likely to experience exhaustion and chronic fatigue [1, 7, 17, 26, 47, 61].
Injuries and musculoskeletal disorders
Long driving hours, without adequate breaks and rest periods, are often associated with an increased risk of musculoskeletal disorders, such as lower back pain, neck pain, knee aches, and general body discomfort [7, 11, 18, 22, 25, 27, 28, 33, 34, 42, 43, 50, 51, 56, 58, 61,62,63]. Furthermore, commercial drivers may be vulnerable to various injuries due to road crashes and ergonomic challenges stemming from prolonged driving [9, 37, 39, 45, 46].
Non-communicable diseases
Cardiovascular health risks [7, 9, 12, 32, 50, 69] and obesity/overweight [7,8,9, 22, 26, 31, 36, 52, 60, 67] have been observed among commercial drivers who were exposed to poor psychosocial work conditions. For example, long driving hours, job strain, and exhaustion are often associated with increased likelihood of ischemic heart disease [59], hypertension [22, 27, 40, 44, 60, 64], and myocardial infarction [37]. Furthermore, there is evidence suggesting that commercial drivers may be at higher risk for conditions such as cancer [69], diabetes [7, 9, 22, 36, 37, 44, 60], kidney disease [22, 39], bladder disorders [22, 27], digestive issues [50], respiratory disorders [22], stroke [22], and haemorrhoids [50], particularly when working in unsafe environments.
Infectious diseases and other health issues
HIV/AIDs has been found among truck drivers in Southern Africa (Zambia, South Africa and Zimbabwe), especially among drivers who drive long distances and spend most days of the month (more than 20 days/month) on the road [37]. Additionally, poor physical health [12, 25, 38] and well-being [13, 16, 21, 23, 53], hearing loss [31], and headache [7] have been observed among commercial drivers, potentially linked to the hostile and precarious nature of their work environment.
Personal risk factors and poor health outcomes
There is evidence suggesting that drivers who are immigrants [34, 43, 70], female [43], married [13], or have no or low levels of education [14, 48], as well as those who are obese or overweight [4, 22, 44, 64, 70], have high cholesterol [9, 22, 44], or are over 40 years, may experience poor psychosocial work factors and related health outcomes. Additionally, risky behaviours and lifestyles such as alcohol consumption and smoking [4, 8, 9, 18, 20, 22, 32, 37, 48, 55, 60, 64], the use of illicit drugs and caffeine [8, 22, 32, 60], poor dietary habits, including fast food consumption and low fruit intake [9, 22, 43, 60], and lack of physical activity [4, 18, 33, 43, 67, 69] are commonly associated with commercial driving and may contribute to poor occupational health outcomes. Furthermore, drivers without health insurance [67, 70], limited access to healthcare [9, 67], those who rely on over-the-counter medications or self-medication [7, 22, 67], and those who delay seeking healthcare [7] may be more vulnerable to impaired health and well-being.
Health promotion interventions
We grouped health promotion interventions into two themes; interventions focused on improving psychosocial working conditions and those focused on the unhealthy lifestyles of the drivers.
Interventions on improving working conditions
A qualitative study conducted among taxi drivers in Canada has shown that using evaluative, placative and entertaining talk are effective protective strategies for avoiding risky trips and preventing unhealthy behaviours such as smoking during trips among drivers [38]. These strategies help commercial drivers to manage the threat to their health and are also sources of social support that help reduce long driving hours [22]. Also, driver unions used education and advocacy for better working conditions and work environment that helped to improve road transport industry’s occupational health and safety issues in Mexico, especially for female commercial drivers [39]. The use of advocacy by female drivers in Mexico had helped created only female taxi stands [39]. In addition, Garbarino and colleagues [8] have shown that enforcing rest stops or rest breaks regulations, working time or driving hours, occupational health and safety standards, and regular surveillance were fundamental approaches to improving working conditions in the road transport industry. Furthermore, a randomised controlled trial among truck drivers in the United Kingdom has shown that once a week whole day time nature helped reduced chronic and acute fatigue among the drivers [47]. However, it is worth noting that spending time in nature did not significantly reduce the depression and anxiety levels of truck drivers. Legislative support for women drivers, using the technological device to track drivers to adhere to rest breaks, taking breaks between trips by taxi drivers and reducing drivers’ workload and putting two drivers on long trips reduced musculoskeletal issues and emotional exhaustion [7, 22, 39].
Interventions on improving healthy behaviours
A longitudinal study in Australia used health promotion campaigns in healthy eating, drinking and physical activity and supply of free fruits to improve eating and drinking behaviours of truck drivers [71]. Also, truckers in Portugal reported that enforcing exercise during rest days in their organisations helped improve their habit of exercising [51]. Evidence shows that workplace campaigns that encouraged eating and exercising at fixed times, using self-control, replacing snacks with fruits, preventing skipping of meals, promoting the consumption of healthy meals, biking to work, parking far away from truck stops to walk, riding during waiting times helped change their risky lifestyles [52]. Similarly, an experiment conducted in China among bus drivers revealed that adding fresh fruits (apples and bananas) decreased depression levels of bus drivers and improved their eating habits [66]. Moreover, evidence from transport drivers in Chile shown that transport companies that provided access to a gymnasium, complementary health check-ups every six months, and access to a physiotherapist and a nutritionist improved the diet, physical activity and occupational well-being of the drivers [60].
link






